WHO Eritrea Supports Maternal Mortality Reduction Efforts
One of the Millennium Development Goals (MDGs) aims at improving maternal health - MDG 5. The two targets of this goal are reducing by three quarters, between 1990 and 2015, the maternal mortality ratio; and achieving, by 2015, universal access to reproductive health.
According to a WHO, UNICEF, UNFPA and World Bank 2012 report, “Trends in maternal mortality: 1990 to 2010”, the annual number of maternal deaths dropped from more than 543,000 to 287,000 – a decline of 47 per cent.
In Eritrea, maternal and child health is one of the priority programmes that constitute the Basic Health Care Package as defined in the National Health Policy and Health Sector Strategic Plan.
Accordingly, the government, in collaboration with partners and stakeholders developed and adopted a Road Map for accelerating the attainment of the MDGs related to maternal and newborn health as a national strategy for addressing the maternal and newborn mortality.
Consequently, out of the 46 countries in the WHO African region that are making progress towards achieving the MDG 5 Eritrea became one of the only two countries that were on track to achieve those targets in 2008.
To support the ongoing efforts, WHO, in collaboration with its partners, is actively involved in providing the necessary support to achieve the goals and objectives of the National Sexual and Reproductive Health (SRH) program.
In line with these ongoing efforts, a task force was established by the government at the end of 2010 to implement the activities set out in the Campaign on Accelerated Reduction of Maternal Mortality in Eritrea (CARMME) that was launched in September 2010 by the Ministry of Health in collaboration with WHO, UNICEF and UNFPA.
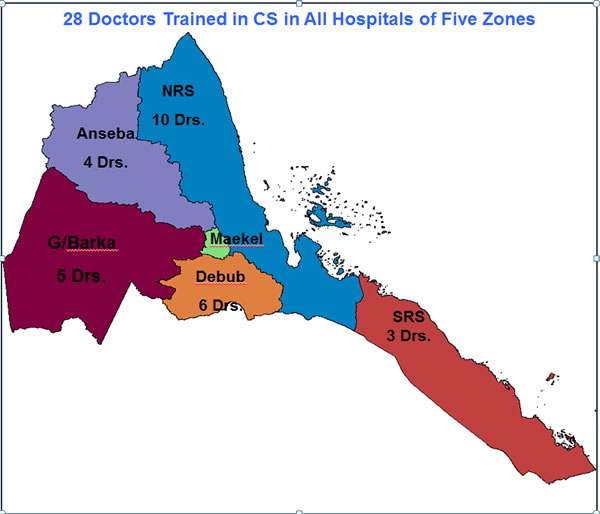
In line with the priorities set out by the task force, to address the identified capacity gaps, the Ministry of Health in collaboration with the WHO Country Office in Eritrea has trained 28 doctors in the provision of comprehensive emergency obstetric and neonatal care (C-EmONC) in eight rounds starting from December 2010 to date.
These trainings which last four to eight weeks each, are being delivered by the obstetrics and gynecology specialists in Orotta Maternity Hospital in Asmara with the financial support of WHO with the objective to empower new graduates who are newly assigned to regional hospitals to decide and perform caesarian section in order to strengthen the comprehensive emergency obstetric and neonatal care (EmONC) services.
Furthermore, in 2011 WHO Eritrea donated various types of reproductive health commodities as well as two vehicles to serve as ambulances in two health facilities in the Gash Barka and Southern Red Sea regions. The donated supplies include items for the health facilities to enhance the maternal/delivery wards in these same regions- the two most hard to reach regions of the country.
Maternity waiting homes (MWH) have been the other key support areas of WHO in the country. Support through MWHs began in 2008 with intervention areas along the Red Sea coastal areas. So far, 11 MWHs have been constructed according to the standard of WHO.
As complementary services to this intervention, distribution of food and other supplies (water tankers, reproductive health commodities, kitchen utensils, etc … were also part of the program.
Consequently, these interventions have contributed to an increased skilled care attendance resulting to more than 97% deliveries which were managed in MWHs in 2010 while less than 3% were referred to higher level facilities.
As a result, only two maternal deaths were reported out of 2,814 deliveries that were carried out in the SRS from 2008 to 2010. Encouraged by the impact of these interventions, some communities have also taken initiatives of building their own MWHs.
Taking into account all the efforts that are underway to improve delivery by skilled birth attendants and improving the availability, timely utilization and quality of emergency obstetric services, and the current emphasis in equipping zonal and community hospitals, Eritrea is likely to achieve much more than was targeted in this MDG.
According to the trends estimated in 2008 Eritrea has already surpassed its 2015 target of 350 scoring 280 in 2008.
The comprehensive EmNOC training includes:
- Caesarian section
- Induction or acceleration of labor
- Blood transfusion and
- Basic EmOC +
The Basic EmOC functions include:
- Administer parenteral antibiotics
- Administer uterotonic drugs (i.e. Oxytocin; Ergometrine; Misoprostol)
- Administer parenteral anticonvulsants for pre-eclampsia and eclampsia. Magnesium sulphate (MgSO4) is the drug of choice
- Perform assisted vaginal delivery (Vacuum, forceps, breech etc.)
- Manual removal of placenta
- Removal of retained products of conception (MVA, E&C)
- Perform basic neonatal resuscitation
Additionally, the following functions are included in the definition of Basic EmOC:
- Set up intra-venous fluids;
- Use of partograph;
- Administer local anaesthesia; and
- Repair of episiotomy and perineal tears.