Bringing healthcare to rural communities
Ndapewa lay awake, listening to the sounds of the night: the leaves of the mopane trees rustling in the light breeze; in the distance, a donkey braying; and in her hut, her husband’s light snoring, and the fast, shallow breathing of her child, Ndakolo.
Ndakolo was now three months old. Ndapewa had made sure that she was near to the district hospital in time for the birth, arriving two weeks before she was due, and camping in a field near to the hospital. This was her first child; the confinement came sooner than expected, and was difficult. But in the end, Ndakolo was born: a small, fine-featured baby, with fingers no thicker than kindling twigs. She had not expected his features to be so delicate: perfectly shaped, almost translucent nails; fine lips sucking on her nipples, labouring to release the unwilling flow of milk.
The nurse had told her at the hospital that at first, Ndakolo would lose some weight – this was normal – but that soon he would start to grow. Now Ndakolo began to stir. She brought his mouth to her nipple, and even though the nipple remained dry, he settled down.
The nurse also said she should bring him back to the hospital if he had a fever, or was breathing very fast, or losing weight. Now, lying awake, Ndapewa wondered: Was his breathing too shallow, and fast? What was “too fast”? And how was she to know if he was gaining enough weight?
If the hospital were nearby, she could easily take Ndakolo in for a check-up. But the village lay deep in the bush, a three-hour walk along the sandy track leading to the potholed, dusty main road. The hospital was a further half-hour’s driving away, if a passing car would stop, and you could pay the twenty dollars that was the standard asking price. Just getting to the hospital would be a strain, on both her and Ndakolo, and she would have to borrow money from friends to pay for a lift. Anyway, she could just be worrying about nothing – Ndakolo was probably fine. The light sweat on his forehead could be unimportant. She would wait a few days and see...
Ndapewa’s dilemma is by no means unique. Rural communities throughout the world face severe challenges in accessing the healthcare services which are traditionally found in regional centres. In a country as vast and sparsely populated as Namibia, this is true even though the healthcare infrastructure is relatively well developed.
If access to primary healthcare is truly a basic human right, primary healthcare must be brought to rural communities.
In Ethiopia, for example, an ambitious community-based Health Extension Programme (HEP) commenced in 2003; to date, over 38 000 Health Extension Workers (HEWs) have been trained and deployed throughout the country. The Ethiopian HEP has been so successful that representatives from several African countries, including Namibia, have visited Ethiopia to study the HEP in action, so that it can be adapted and applied at home.
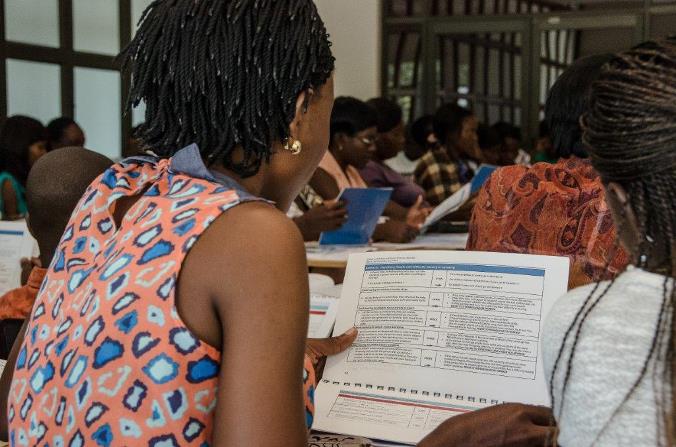
In Namibia, the Health Extension Workers (HEW) programme commenced with a pilot programme in 2012. This was followed by the first multi-regional HEW training in 2013 – 2014. For the 2014 – 2015 HEW training cycle, about 900 trainees have been recruited from ten regions. They must have passed Grade 10, with at least a D symbol in English. In addition, candidates are selected from villages in consultation with the community members and leaders. The current group of trainees will bring the total number of HEWs to 1 200. As far as possible, they will work in their own villages. This arrangement helps to ensure that there is a close relationship between HEWs and the communities they serve.
The Village Health Committee (VHC) members supervise and monitor the work of the HEWs, and alert them to pregnancies in the community, and to other community members in need of attention. The extent of community support for the HEW programme is obvious, in no small part because the VHC represents the interests of communities and traditional authorities.
The World Health Organization (WHO) is well acquainted with the background to the Ethiopian HEP, and the profound impact it is having in that country. Because Ndapewa’s plight is essentially the same as that of members of isolated communities in Ethiopia, and indeed worldwide, WHO joined hands with the MHSS to make the HEW programme a reality in Namibia. According to Dr Mary Brantuo, the WHO Child and Adolescent Health Officer in Namibia, “The health extension programme is training and empowering young men and women with knowledge and skills to make a difference in their communities. They will serve as agents of change to improve health outcomes in individuals, families and communities.”
The lessons learnt in Ethiopia are important for other African countries, including Namibia. H.E. Dr Kesetebirhan Admassu, the Ethiopian State Minister of Health offered three pieces of advice:
“One: Go to scale as quickly as possible if you want to see an impact.”
In Namibia, the MHSS has already moved on from the 2012 pilot programme to the current full-scale HEW training programme. The goal of the MHSS is to roll out HEW services throughout the country.
“Two: Be ambitious. Most people thought that training 30 000 health extension workers was an impossible feat. … we not only did it, we surpassed that number!”
The MHSS has estimated that providing quality HEW services to all rural communities in Namibia will require at least 4 000 HEWs. Going forward, monitoring and supervision of HEWs (by both VHCs and the MHSS), ongoing training to ensure that the corps of HEWs remains at appropriate levels, and ensuring that their supplies are always replenished, will be crucial.
“Three: Own the process. Determine what you want to do and rally your forces to help you do what you set out to do.”
What do HEWs currently do? And should they be expected to do more in the future? The HEW training covers community mobilisation, basic first aid, community-based maternal and newborn care and integrated child health, HIV and AIDS, TB and malaria, and social welfare and disabilities. HEWs may only provide non-prescription medication to reduce fever and pain as a temporary measure, if they have referred a case to the clinic or hospital. They are not trained doctors or nurses, and they will never replace them. They provide important basic care and information, and can alert the MHSS to developments on the ground. However, it will be essential to guard against overloading them with an ever-increasing burden of responsibilities, as doing so would compromise the important services they provide.
What difference would an HEW in Ndapewa’s village have made?
When Ndapewa makes the decision not to take Ndakolo to the clinic, she unwittingly places his life at risk. If there was an HEW providing primary healthcare in her village, the HEW would have known about her case. She would have monitored Ndakolo’s progress, taking his temperature, measuring his breathing rate, and weighing him. She would have known if he was failing to gain weight, or even losing weight and condition. She would have realised if Ndapewa was struggling to produce enough milk for Ndakolo. And she would have referred his case to the clinic or hospital.
It is easy to understand why mothers in Ndapewa’s situation make the mistake of choosing not to take their babies to the hospital. Travelling from a rural village to a regional centre can take time, and effort, and money. And it is true that babies like Ndakolo may get better without medical attention.
But it is also true that they may become seriously ill, and die.
Preventing tragedies such as this, and bringing a broad array of positive healthcare benefits directly to rural communities, is the ultimate goal of the HEW programme in Namibia.
Dr Monir Islam, the WHO Country Representative in Namibia, regards the HEW programme as an essential component of health services in rural areas, particularly for mothers and their babies: “Improved community awareness and skills in maternal and child health is one of the expected results of the PARMaCM programme. HEWs are crucial in realising this result, which is why WHO attaches great importance to their training.”